
Have you ever felt like food is getting stuck in your chest? Maybe it happens with solids, or maybe even liquids. You might feel a strange pressure, or perhaps sharp pain that feels eerily similar to a heart attack. If this sounds familiar, you are not alone, but you might also be frustrated. Many people spend years being told they have acid reflux (GERD) when the real culprit is something else entirely: an esophageal motility disorder, which is a condition where the muscles of the esophagus do not contract properly to move food into the stomach.
We often think of swallowing as automatic. It just works. But behind that simple act is a complex dance of muscle contractions called peristalsis. When that rhythm breaks down, life becomes difficult. Eating stops being a pleasure and starts becoming a source of anxiety. The good news? We now have better tools than ever to diagnose these issues. Specifically, a test called high-resolution manometry (HRM) allows doctors to see exactly what your esophagus is doing, rather than guessing. Let’s break down what these disorders are, how we find them, and what you can do about them.
What Are Esophageal Motility Disorders?
Your esophagus is a muscular tube connecting your throat to your stomach. For food to travel down smoothly, two things must happen perfectly. First, the muscles in the body of the esophagus must squeeze in a coordinated wave (peristalsis). Second, the lower esophageal sphincter (LES)-the valve at the bottom-must relax to let food in, then close tight to keep stomach acid from coming back up.
Motility disorders mess up this process. They fall into two main buckets:
- Primary Disorders: These start in the esophagus itself. The nerves or muscles controlling the tube are damaged or malfunctioning. Examples include achalasia and diffuse esophageal spasm.
- Secondary Disorders: These are caused by other systemic diseases. For instance, scleroderma (a connective tissue disease) affects about 80% of patients’ esophages, causing the muscles to weaken and scar over time.
The most common symptom across all these conditions is dysphagia, which means difficulty swallowing. But it’s not just about choking. You might experience regurgitation of undigested food, unexplained weight loss, or chronic chest pain. In fact, chest pain from esophageal spasms is so intense that many patients end up in emergency rooms thinking they are having a heart attack. Once cardiac causes are ruled out, the focus shifts to the gut.
The Gold Standard: High-Resolution Manometry
If you have trouble swallowing and an endoscopy (camera test) shows no physical blockage like a tumor or stricture, your doctor will likely order a motility test. For decades, doctors used standard manometry, which gave a blurry picture. Today, the gold standard is high-resolution manometry (HRM).
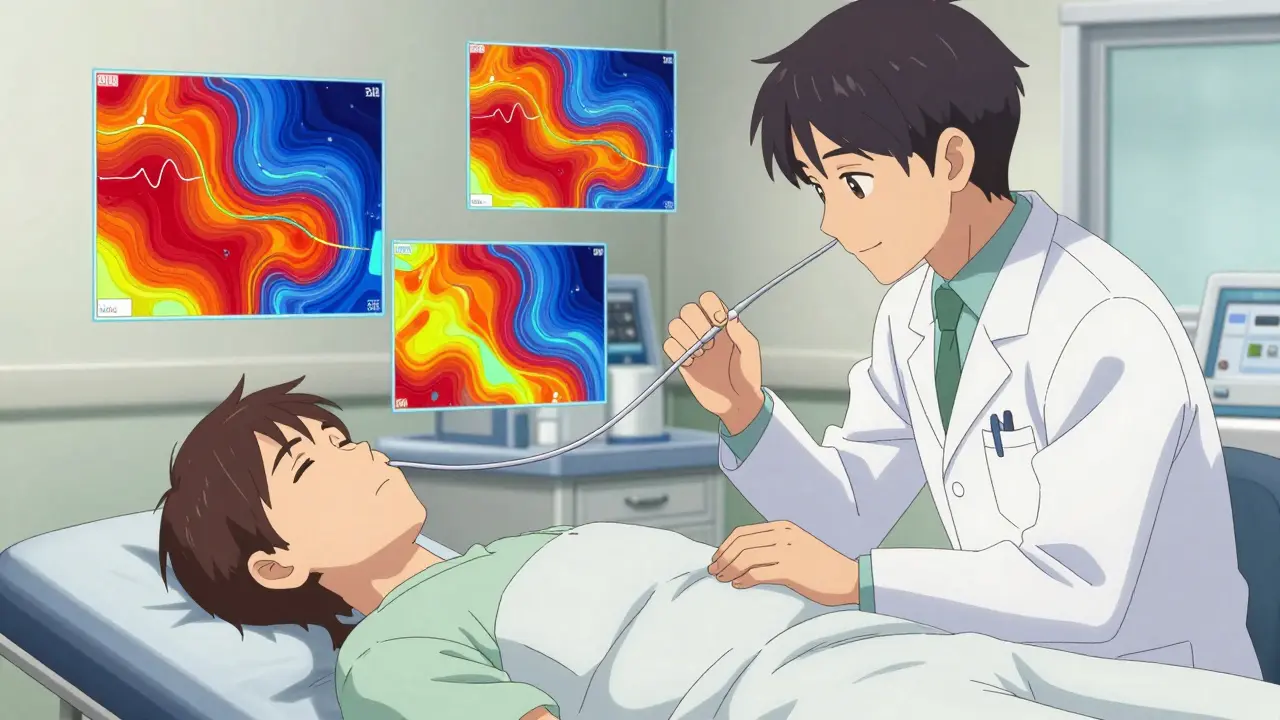
So, what actually happens during HRM? You’ll swallow a thin, flexible catheter through your nose. This isn’t pleasant, but it’s usually manageable. The catheter has 36 sensors spaced evenly along its length. As you swallow water, these sensors measure pressure changes in real-time. The result is a colorful topographic map of your esophagus’s activity.
This map tells the doctor three critical things:
- How strong are the contractions?
- Are they coordinated (moving in the right direction)?
- Does the lower esophageal sphincter (LES) relax fully?
Without HRM, diagnosing specific disorders was like trying to read a book in the dark. With it, doctors can pinpoint exactly where the breakdown occurs. Studies show HRM has a sensitivity rate of 96% for diagnosing achalasia, compared to just 78% for traditional barium swallows.
Understanding the Diagnosis: The Chicago Classification
Raw data from manometry is complex. To make sense of it, gastroenterologists use a standardized system called the Chicago Classification. This is a diagnostic framework that categorizes esophageal motility disorders based on manometric findings. The current version, v4.0, was published in 2023. It divides disorders into "major" (requiring treatment) and "minor" (possibly normal variants).
Here are the most common major diagnoses you might encounter:
| Disorder | What Happens | Key Symptom |
|---|---|---|
| Achalasia | The LES fails to relax, and the esophagus loses its ability to push food down. It’s like a door that won’t open and a conveyor belt that stopped working. | Dysphagia to both solids and liquids; regurgitation. |
| Diffuse Esophageal Spasm (DES) | Uncoordinated, chaotic contractions. Some parts of the esophagus squeeze while others don’t. | Chest pain; intermittent dysphagia. |
| Jackhammer Esophagus | Hypercontractile disorder. The esophagus squeezes way too hard (pressures >5000 mmHg•s•cm). | Severe chest pain; dysphagia. |
| EGJ Outflow Obstruction | The LES doesn’t relax enough, but the esophagus still tries to push food down. Often seen in early achalasia or post-surgery. | Dysphagia; chest discomfort. |
Achalasia is the most well-known primary disorder. It affects about 1 in 100,000 people annually. It is further split into three types based on the manometry pattern: Type I (no contraction), Type II (pan-esophageal pressurization, the most common at 70%), and Type III (spastic contractions). Knowing the type matters because it influences which treatment will work best for you.
Why Do Patients Get Misdiagnosed?
You might be wondering why it takes so long to get answers. A survey by the International Foundation for Gastrointestinal Disorders found that 68% of patients experienced diagnostic delays of 2 to 5 years. Why?
The biggest reason is misattribution. Symptoms like chest pain, heartburn, and difficulty swallowing overlap heavily with GERD (gastroesophageal reflux disease). Doctors often prescribe proton pump inhibitors (PPIs) first. If the PPIs don’t help, the patient is often sent home with advice to "eat slower" or "avoid spicy foods."
Dr. Kristle Lee Lynch from the University of Pennsylvania notes that many patients are treated for GERD for years before the underlying motility issue is found. This is dangerous because treating a motility disorder with acid reducers doesn’t fix the mechanical problem. In some cases, like jackhammer esophagus, acid suppression might even mask symptoms without addressing the painful spasms.
Another hurdle is access. High-resolution manometry requires expensive equipment ($50,000-$75,000 per system) and specialized training to interpret. While 95% of academic centers in North America and Europe have HRM, less than 10% of facilities in low-income countries do. This gap means many patients simply never get tested.
Treatment Options: Restoring Function
Once diagnosed, the goal is to relieve the obstruction or calm the spasms. Treatment depends entirely on the specific disorder.
Treating Achalasia
Since the LES won’t open, we need to physically weaken it. There are three main approaches:
- Laparoscopic Heller Myotomy (LHM): A surgeon cuts the muscle fibers of the LES through small incisions in the abdomen. Success rates are 85-90% at 5 years. It’s often combined with a partial fundoplication to prevent reflux.
- Peroral Endoscopic Myotomy (POEM): This is a newer, less invasive procedure. The doctor uses an endoscope to cut the muscle from inside the esophagus. POEM is equally effective as LHM but carries a higher risk of reflux esophagitis (44% vs. 29% at 2 years).
- Pneumatic Dilation: A balloon is inserted and inflated to stretch the LES. It’s less invasive but often requires repeat sessions. About 25-35% of patients need another dilation within five years.
Treating Spastic Disorders (DES, Jackhammer)
For disorders involving too much squeezing, the approach is different. Medications like calcium channel blockers or nitrates can relax smooth muscle, but side effects like headaches and dizziness are common. Botulinum toxin (Botox) injections into the esophageal muscle can provide temporary relief. In severe, refractory cases, surgeons may perform a myotomy or even remove part of the esophagus, though this is rare.
Emerging Technologies
Innovation is moving fast. Wireless motility capsules (like the SmartPill) allow for ambulatory testing over 24-48 hours, giving a more natural picture of function. AI-assisted interpretation tools are also entering the field, with studies showing 92% accuracy in identifying achalasia patterns-potentially reducing human error. Additionally, magnetic sphincter augmentation devices (like LINX) are being explored for select achalasia patients who still have some peristaltic function.
Living with a Motility Disorder
Getting a diagnosis is a relief, but living with the condition requires adaptation. Here are practical tips that many patients find helpful:
- Modify Your Diet: Chew food thoroughly. Cut meat into small pieces. Avoid dry, tough foods like steak or bread if they trigger sticking sensations. Warm liquids can sometimes help relax the LES.
- Eat Slowly: Rushing overwhelms the esophagus. Take smaller bites and wait between mouthfuls.
- Stay Upright: Don’t lie down immediately after eating. Gravity helps move food down, especially if your peristalsis is weak.
- Manage Stress: Anxiety can worsen spasms. Techniques like deep breathing or mindfulness may reduce the frequency of chest pain episodes in DES patients.
Support groups, such as those hosted by the Esophageal Disorders Society, can be invaluable. Hearing from others who have undergone POEM or myotomy can demystify the surgery and reduce fear.
Frequently Asked Questions
Is high-resolution manometry painful?
Most patients describe it as uncomfortable rather than painful. The catheter passes through the nose and throat, which can cause gagging or a feeling of fullness. However, the procedure only takes about 30 minutes, and numbing spray is used beforehand. About 35% of patients report significant discomfort, but satisfaction rates jump to 78% when patients receive thorough pre-procedure education.
Can esophageal motility disorders be cured?
It depends on the disorder. Achalasia cannot be "cured" in the sense that the nerve damage is permanent, but treatments like myotomy or POEM can effectively manage symptoms for many years. Spastic disorders like DES may come and go, and medications can control symptoms, but there is no definitive cure. Secondary disorders depend on managing the underlying systemic disease.
What is the difference between achalasia and EGJOO?
Both involve difficulty relaxing the lower esophageal sphincter (LES). In achalasia, the esophagus also loses its ability to contract (peristalsis is absent or ineffective). In EGJ Outflow Obstruction (EGJOO), the esophagus still contracts normally, but the LES doesn't open enough. EGJOO can be a sign of early achalasia or a result of previous surgery.
Why did my doctor recommend an endoscopy before manometry?
Endoscopy is the first-line test to rule out structural problems like tumors, strictures, or eosinophilic esophagitis. Manometry tests function, not structure. You need to ensure there isn't a physical blockage before assessing how well the muscles are working. Guidelines from the American College of Gastroenterology recommend this sequence.
Can stress cause esophageal motility disorders?
Stress does not cause primary motility disorders like achalasia, which are neurological. However, stress can significantly worsen symptoms in functional disorders like diffuse esophageal spasm or non-specific motility issues. Anxiety can heighten pain perception and trigger spasms, making management harder.
What is the Chicago Classification v4.0?
It is the latest international standard for interpreting high-resolution manometry results, published in 2023. It categorizes disorders into major (requiring treatment) and minor (possibly normal variants) groups. This system improves diagnostic accuracy and ensures doctors worldwide use the same criteria, reducing misdiagnosis.
Brett Webster
June 9, 2026 AT 12:17As a gastroenterologist, I appreciate the clarity of this breakdown. High-resolution manometry is indeed the game changer we needed. For years, we were flying blind with standard tests, and it led to countless misdiagnoses of GERD when the real issue was motility. The Chicago Classification v4.0 has standardized our approach significantly, allowing for more precise treatment plans like POEM versus Heller Myotomy based on specific achalasia types.
Callie Skipper
June 9, 2026 AT 19:28im so glad i found this because i have been having chest pains for months and my doctor just keeps giving me omeprazole. it feels like something is stuck every time i eat solids but liquids are fine sometimes. maybe i need that tube test?
Brett Webster
June 10, 2026 AT 02:12Callie, please do not ignore those symptoms. Dysphagia to solids is a red flag that requires investigation beyond acid suppression. If your endoscopy was clear, ask specifically for high-resolution manometry. It is uncomfortable but necessary to rule out structural issues or motility disorders like achalasia or EGJOO. Early diagnosis prevents complications like aspiration pneumonia.
Lee Coates
June 11, 2026 AT 00:11Typical American healthcare drama :P We spend $75k on machines while people in other countries die without basic care. But sure, let's talk about colorful maps of esophagus pressure instead of fixing the broken system. Enjoy your fancy catheters while the rest of us wait in line for three years.
Miranda River
June 12, 2026 AT 20:50Look, its not all doom and gloom ok? The tech is cool but you guys always forget the human element. Like, who wants a tube up their nose? Its gross. And dont get me started on the cost. Insurance denies it half the time saying its experimental even though its been around forever. Typical bureaucracy at its finest lol.
Brandon Brodsky
June 13, 2026 AT 18:56I had POEM done last year for Type II Achalasia. Let me tell you, the recovery was brutal. Reflux became my new best friend. The article mentions the 44% risk of reflux esophagitis, which is no joke. You trade swallowing difficulty for heartburn that never goes away unless you take PPIs forever. It's a lose-lose situation disguised as a miracle cure.
Christina S.
June 14, 2026 AT 22:20Brandon, I hear you. The reflux after POEM can be tough. However, many patients find that the relief from dysphagia outweighs the manageable reflux. Working closely with your GI specialist to adjust medication can help. It's not perfect, but being able to eat normally again is huge for quality of life. Don't give up hope!
Sherry Wheeler
June 16, 2026 AT 21:03This article is a beacon of light for those of us suffering in silence! 😭 I spent five years thinking I was crazy because the pain felt like a heart attack but the EKG was normal. Finally getting diagnosed with Diffuse Esophageal Spasm changed everything. Understanding that stress triggers spasms helped me start therapy alongside medication. You are not alone in this struggle!
shreya sinha
June 17, 2026 AT 14:51It is profoundly disheartening to observe how medical professionals continue to prioritize pharmaceutical interventions over comprehensive diagnostic evaluations. The fact that sixty-eight percent of patients endure delays of two to five years reflects a systemic failure of empathy and diligence within the healthcare community. One must question the ethical implications of prescribing proton pump inhibitors indiscriminately without ruling out mechanical obstructions, thereby subjecting patients to prolonged suffering under the guise of convenience.
Ganesh Honikol
June 18, 2026 AT 05:03Well said Shreya, the delay in diagnosis is truly unacceptable :(( From my experience in India, access to HRM is still limited to major metro cities. Many rural patients suffer silently. However, awareness is growing. Doctors are now more likely to consider motility disorders if PPIs fail. We need more training centers to interpret these complex manometry charts accurately so that every patient gets the right care regardless of location :)
Hailey Dunston
June 19, 2026 AT 10:04You all seem to miss the point entirely. The issue isn't just the test, it's the interpretation. Most GIs are generalists who barely understand the Chicago Classification nuances. They see a spasm and call it DES, missing Jackhammer patterns. Without specialized expertise, the expensive machine is useless. It’s a classic case of buying the tool but lacking the skill to wield it properly. 🙄
AnneKatherine Stiekes
June 20, 2026 AT 02:06i think the diet tips are really helpful too. chewing food thoroughly seems simple but when you are stressed about eating it is hard to remember. staying upright after meals makes such a difference for me. gravity is your friend here
Glenn Davis
June 20, 2026 AT 22:27Access gap is real. US needs to stop importing cheap doctors and train locals properly. Healthcare is failing everyone.